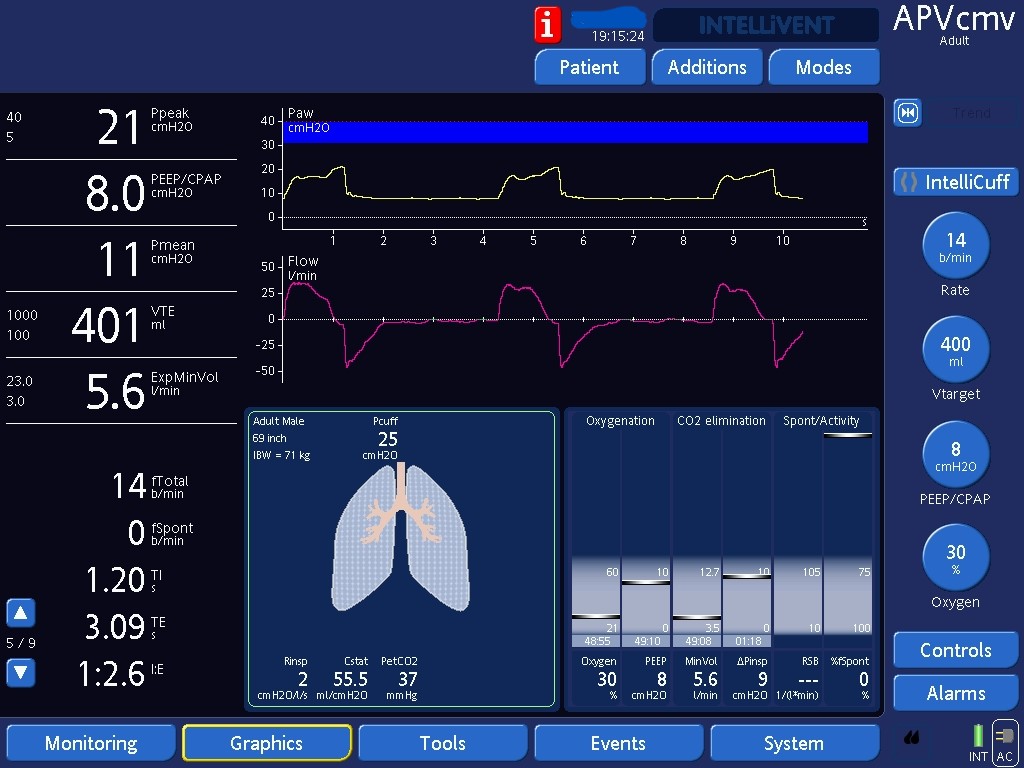
Work Shifting on PRVC (same as APV)
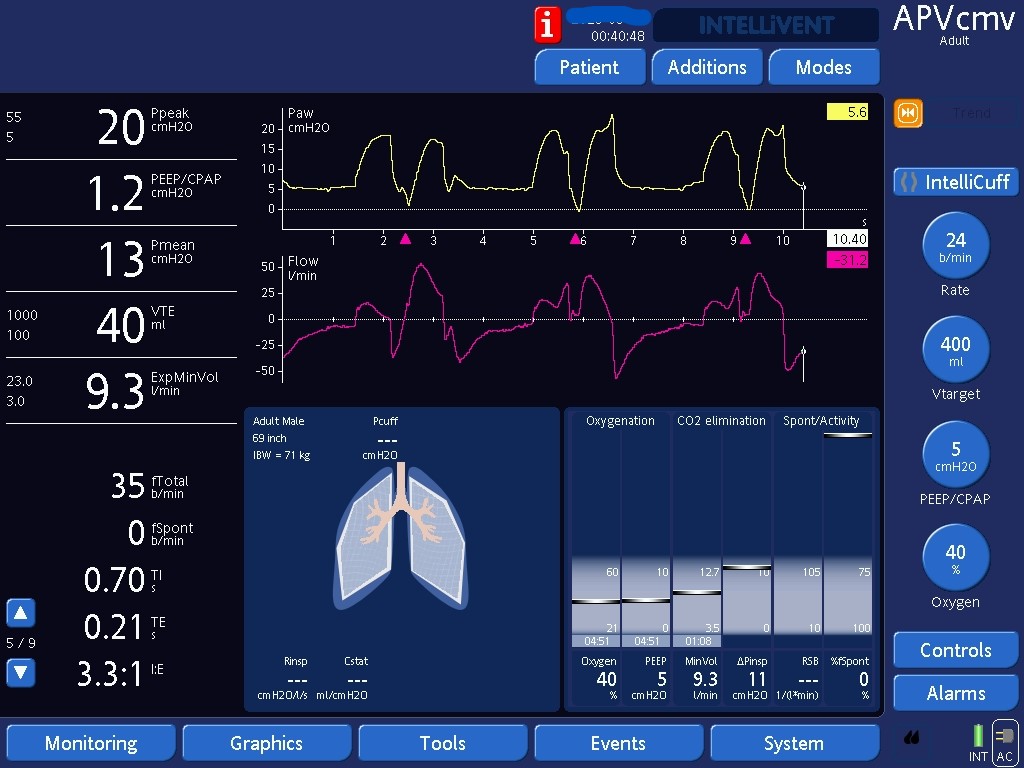
Detecting under-support from work shifting, and the options for shifting work back from the patient to the ventilator.

Detecting under-support from work shifting, and the options for shifting work back from the patient to the ventilator.