Additional Case of Early Trigger Highlighting the Principles of Treatment of this Dyssynchrony
A second early-triggering case reinforcing the core principle of treatment — letting the patient initiate their own breaths.
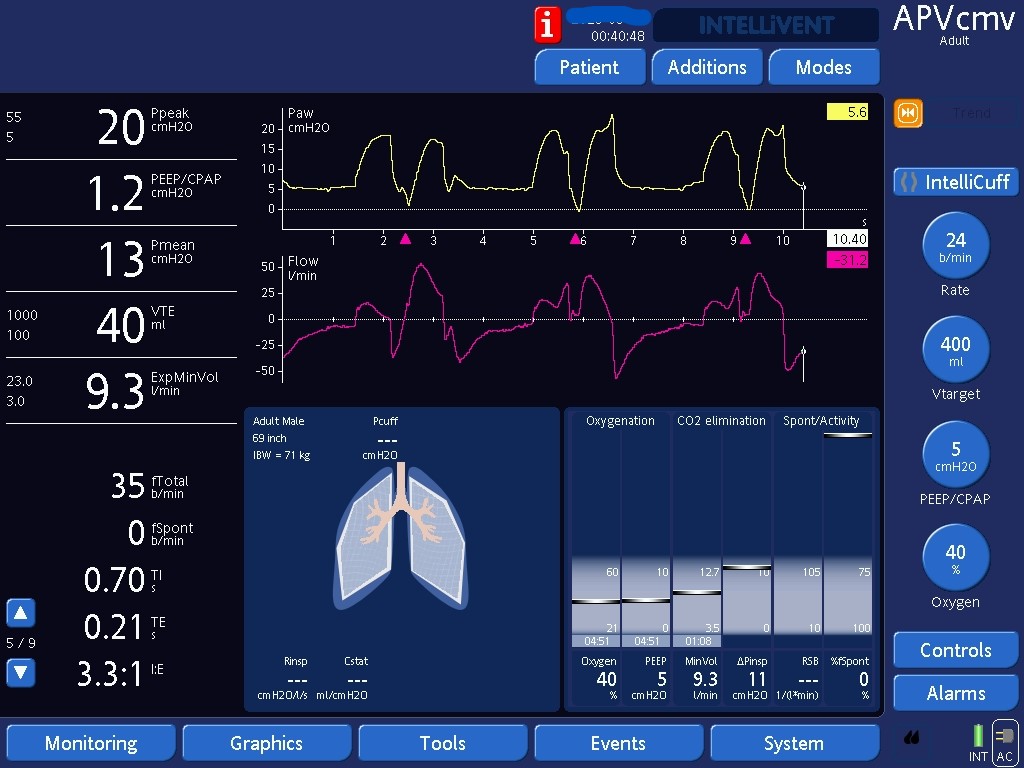

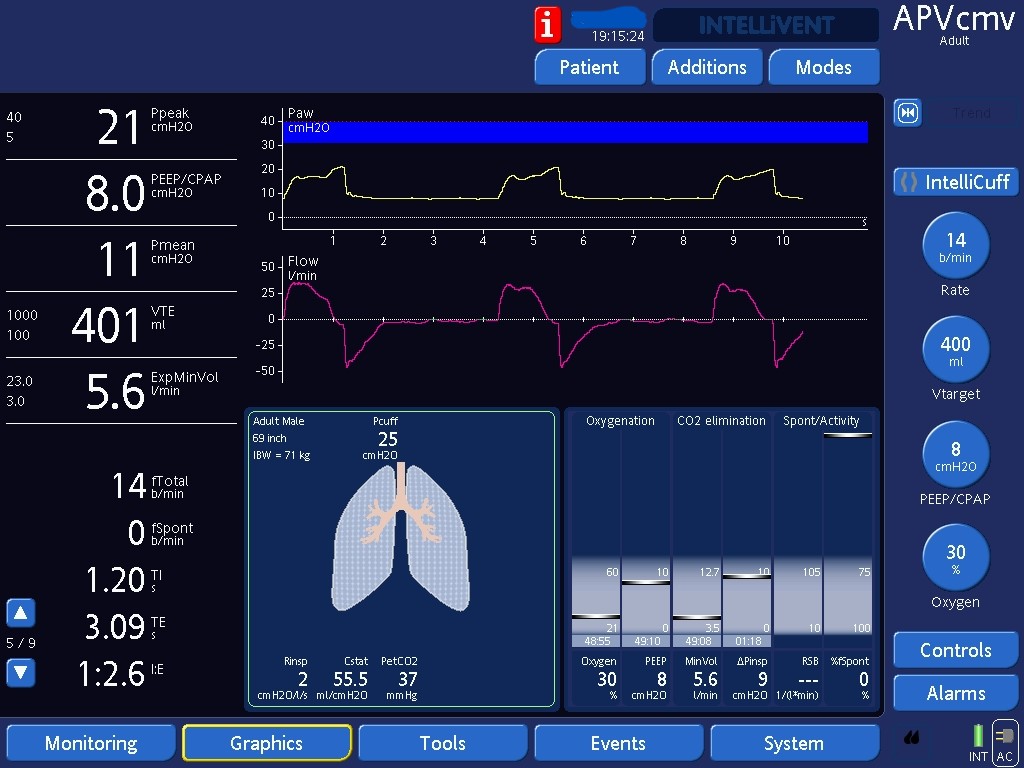
Note how double triggering only occurs after ventilator-initiated breaths (first set of breaths). Double triggering due to early triggering does not happen if the patient initiated the breath (last few breaths) - early triggering is the phenomenon in which the ventilator triggers the breath before the patient starts exerting inspiratory effort. This observation highlights the basis of treatment of this dyssynchrony: allowing the patient to initiate their own breaths. We can accomplish this by decreasing sedation and decreasing the rate/switching mode to pressure support. If these are not possible (e.g., severe ARDS), we may need to increase the depth of sedation or even paralyze the patient if we want to suppress early triggering.

Dropping the set rate gives the patient the opportunity to trigger their own breaths. This is an effective way of treating this dyssynchrony.

Early trigger will only occur if the ventilator triggers breaths, which does not happen in PSV.