Work Shifting
How work shifts from the ventilator to the patient in adaptive-pressure and volume-control modes as patient effort rises.
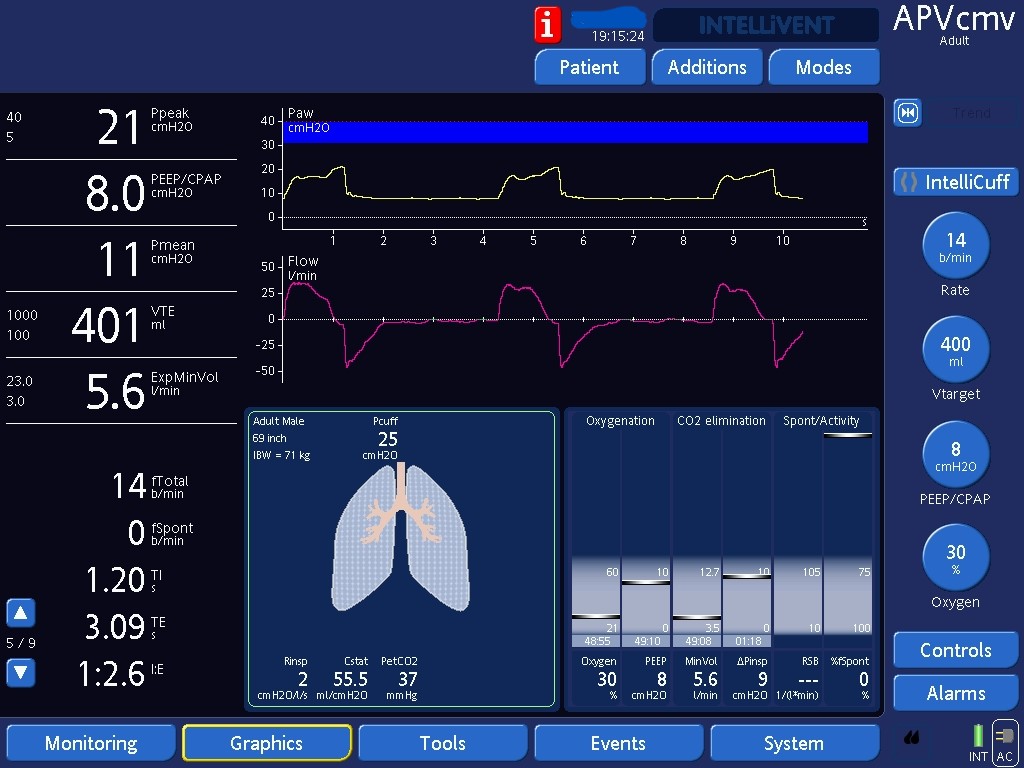
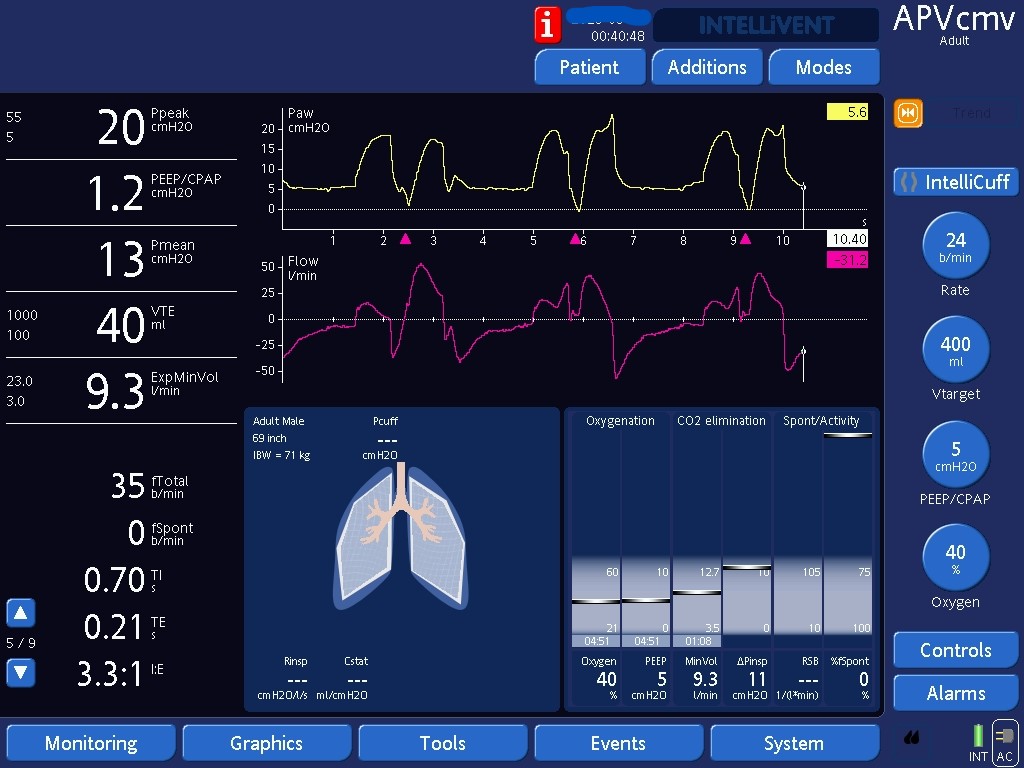
Work shifting may happen in pressure-controlled modes with adaptive targeting schemes (APV, PRVC, Autoflow, VC+…) because the ventilator down titrates the amount pressure it applies above PEEP whenever tidal volumes are higher than target. Therefore, if the patient does more work getting higher tidal volumes than the set target, the ventilator will apply lower pressures to decrease tidal volumes back to target. The more work the patient does, the less work the ventilator does (work shifts from the ventilator to the patient).
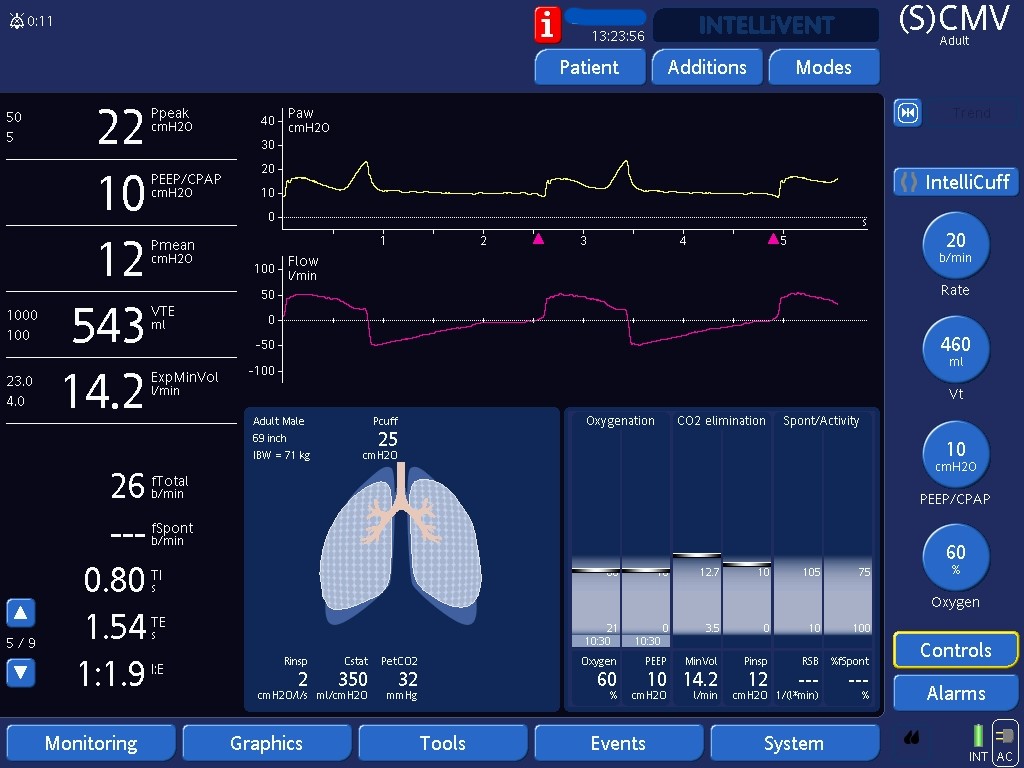
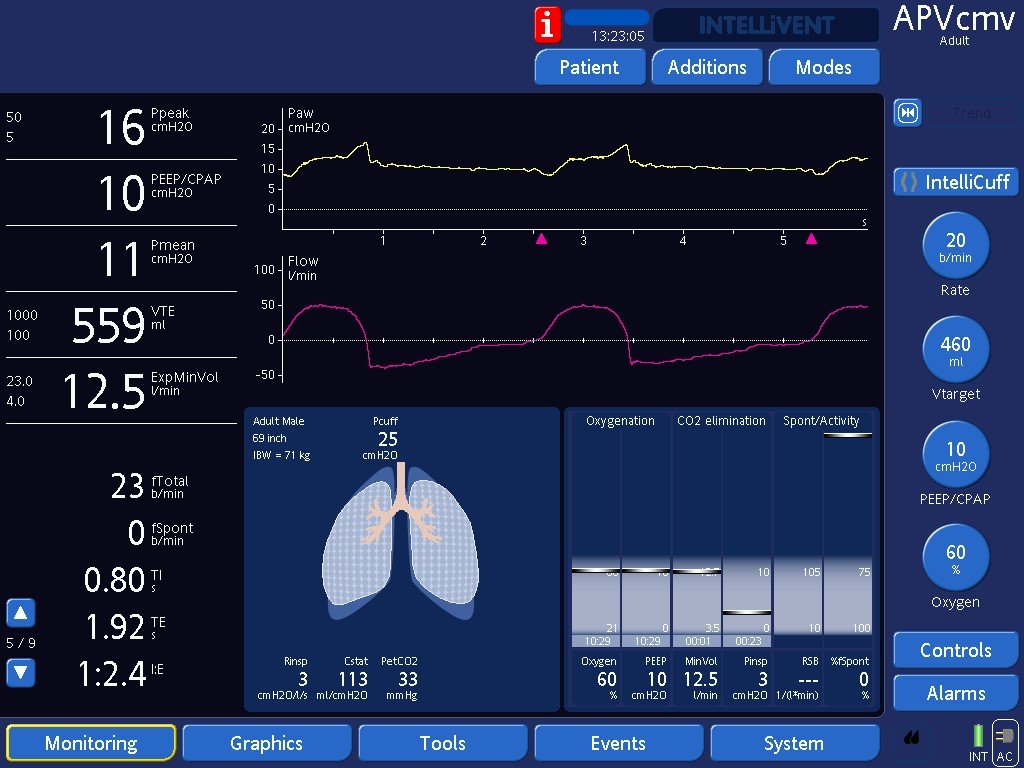
Work shifting also happens in VC. Since flow is the limit variable in VC, the more effort the patient does, the less pressure the ventilator will have to apply to achieve its target flows. This relationship also leads to work shifting. Note the mid-inspiratory scooping in the pressure over time waveform, also called flow dyssynchrony. The patient exerts more inspiratory effort in an attempt to get higher inspiratory flows. However, in VC the ventilator controls flows and will not allow higher flows to be delivered. Hence, airway pressures drop in response to increases in patient inspiratory effort. The treatment of flow dyssynchrony involves increasing inspiratory flows. Some ventilators will allow the user to change flow rates. In others, like this Hamilton ventilator, flows are determined by the set tidal volume and the inspiratory time. To increase flows here, one would either increase tidal volumes and/or decrease inspiratory time.