Troubleshooting Increased Work of Breathing Seen with Modes Using an Adaptive Targeting Scheme
A sedation-free approach to increased work of breathing on an adaptive mode: raise the tidal-volume target or switch to pressure control.
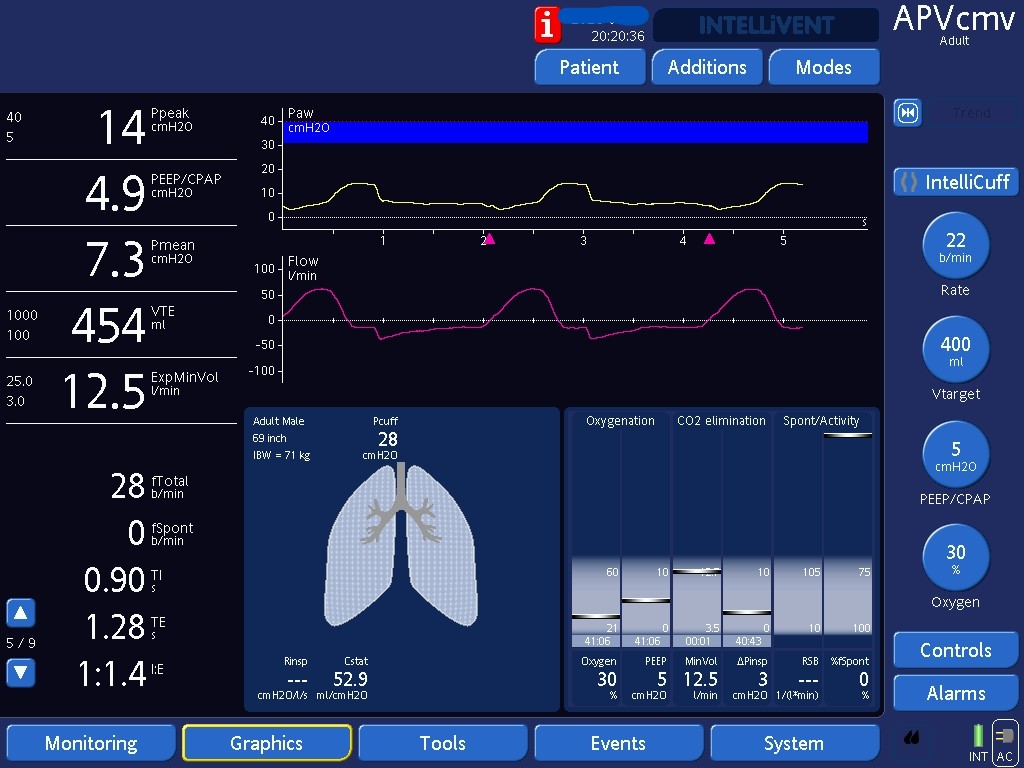

After increasing the target tidal volume from 400 mL to 550 mL, the ventilator is now required to deliver more pressure to meet the higher tidal volume goal. As a result, the inspiratory pressure support has increased (ΔPinsp now 11 cmH₂O instead of 3 cmH₂O). With more support from the ventilator, the patient’s work of breathing decreased as inspected at bedside. Another marker that her respiratory drive decreased is the drop in her RR from 28 in the prior picture to 23 here. This patient did not have ARDS and was intubated for airway protection. Keeping higher tidal volumes, in the range of 8ml/kg of predicted body weight, was therefore thought to be appropriate.
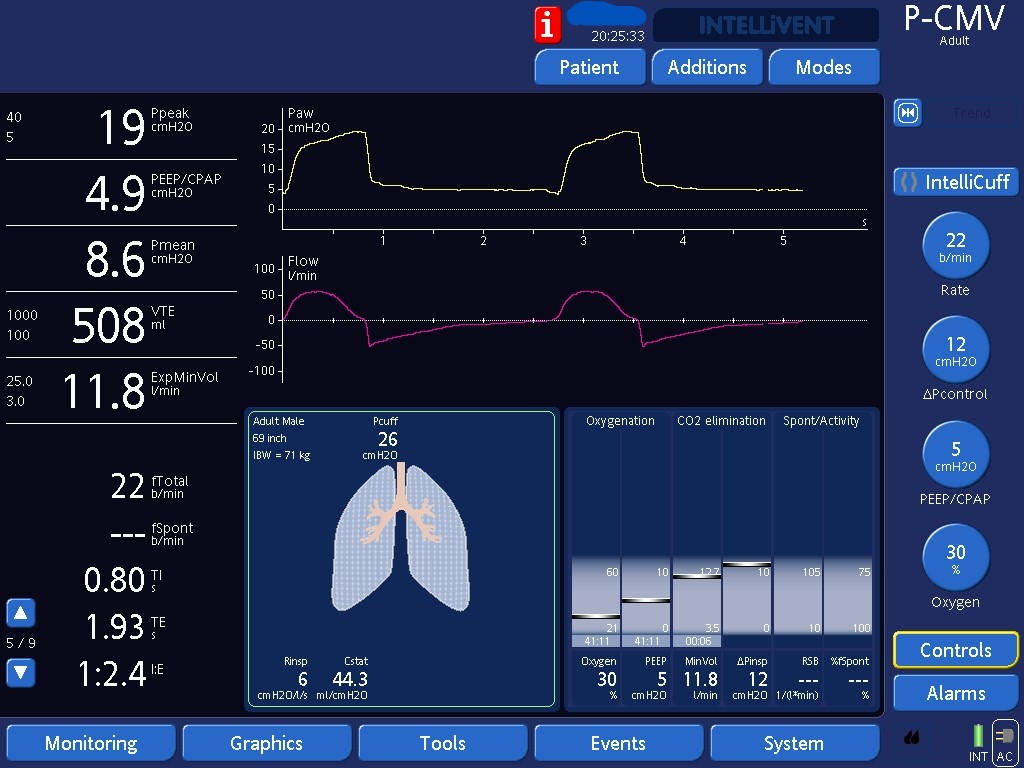
Alternatively, we can switch the patient to Pressure Control. Since we set the amount of pressure given above PEEP (here ΔPcontrol of 12 cmH₂O), work shifting will not occur. The ventilator does not change the amount of work it does in response to patient’s changes in their work of breathing.

When transitioning a patient to Pressure Control (or Pressure Support), it is essential to ensure that the alarm limits are appropriately set since we cannot guarantee a certain tidal volume. Any changes in respiratory system mechanics (e.g., ETT kink) or in patient effort (e.g., after a sedative bolus) may lead to significant drops in tidal volumes. In this example, actual minute volume is 11L/min. Setting a lower limit for the alarm to a value closer to the current minute volume (e.g., 8L/min) will notify us early about a potentially dangerous drop in minute ventilation. Keeping the alarm at 3L/min would be inappropriate, since it could expose the patient to long periods of significant hypoventilation before setting off the alarm.

In this case, we have changed the alarm to 7L/min so it will notify us early about a potentially dangerous drop in minute ventilation.