Late Cycle in Pressure Support
Recognizing late cycling in pressure support and shortening inspiration by raising the expiratory trigger sensitivity.

In pressure support ventilation, there is no direct control for inspiratory time. Instead, inspiration ends when inspiratory flow drops to a preset fraction of its peak, this is known as the Expiratory Trigger Sensitivity (ETS). Increasing ETS ends inspiration earlier. If inspiration is ending too late, raising the ETS shortens inspiratory time. Physiologically, as the patient generates strong inspiratory effort, inspiratory flow remains high. When the patient relaxes their inspiratory muscles, flows fall and eventually meet the ETS threshold, cycling the ventilator to expiration. Typical starting values are around 25%.

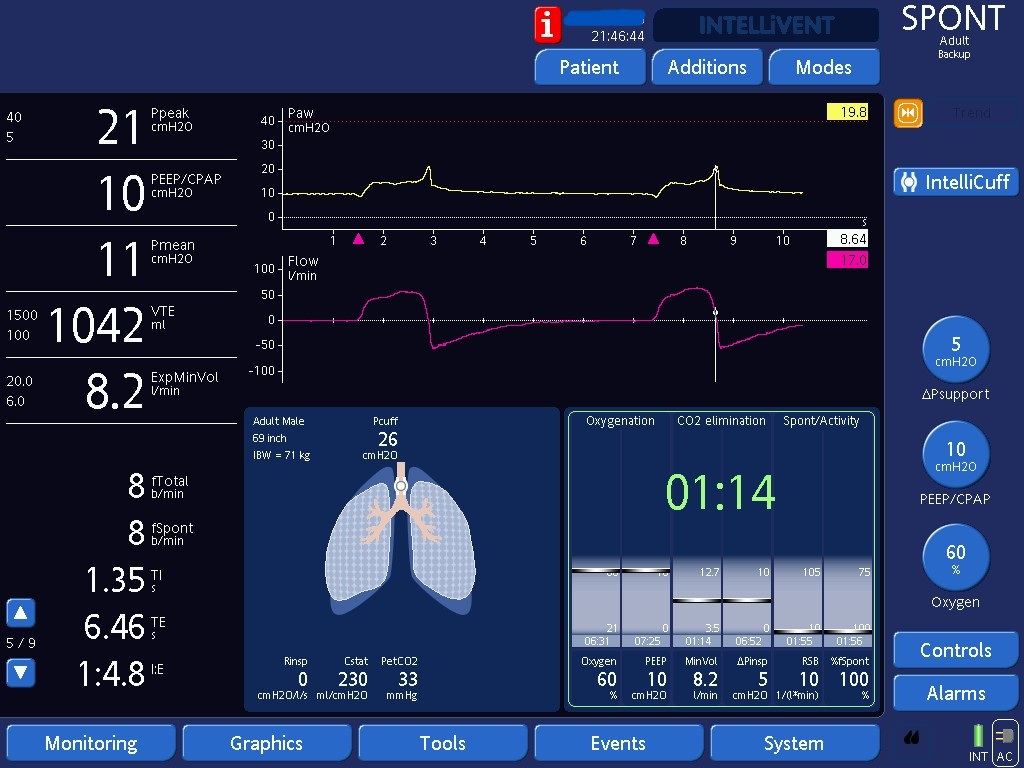
By increasing the percentage of peak flows at which the ventilator cycles the breath, duration of inspiration shortens. Here we are telling the ventilator to end inspiration when inspiratory flows drop from peak to 60%, which is earlier than when flows would reach 25% of peak.
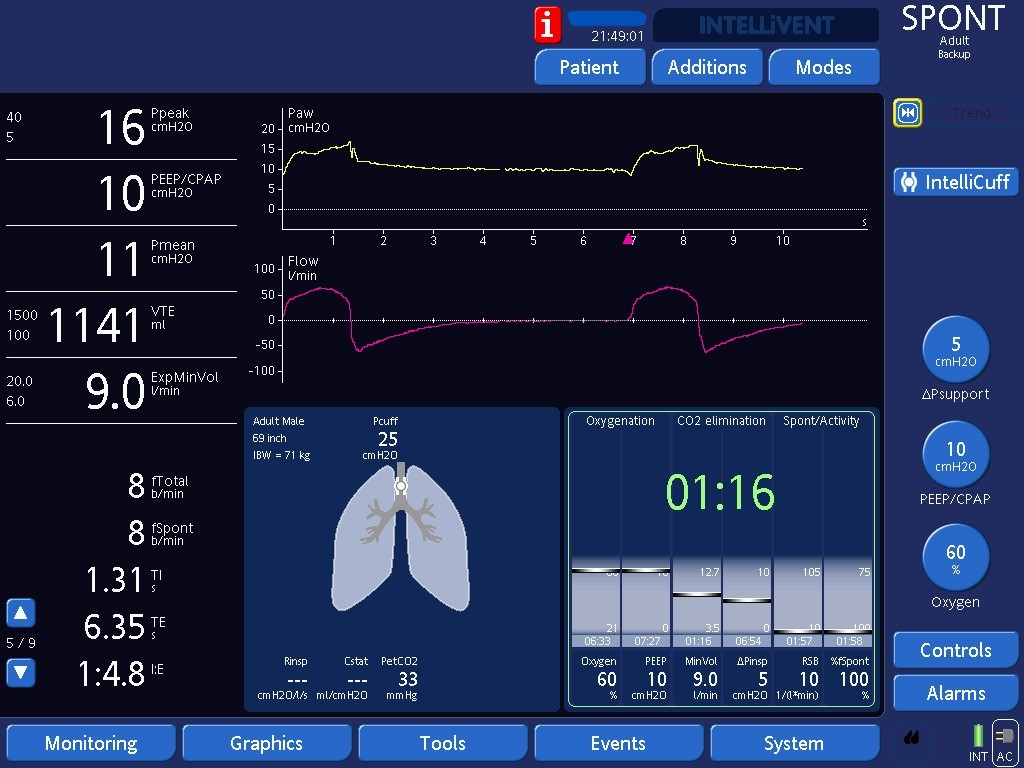
After increasing the percentage of peak flows to cycle the breath from 25 to 60%, note that the late peak disappeared. It is hard to say how clinically significant and how necessary this adjustment was without inspecting the patient and seeing if they looked uncomfortable. Remember, we should treat patients and not waveforms.