Flow Dyssynchrony/Work Shifting in VC Square Flow with Troubleshooting
Diagnosing flow dyssynchrony off the pressure–time waveform in volume control, and managing it.


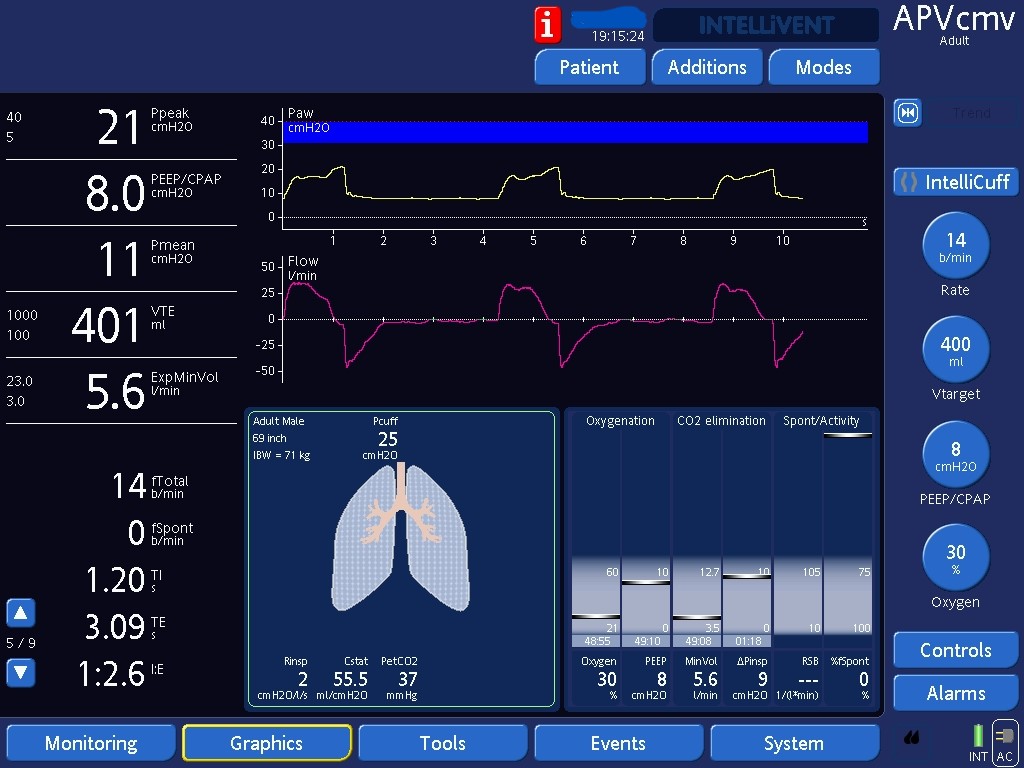
Here you can see how waveforms would look like on VC with constant or square inspiratory flows (we set the flow pattern) in passive patients.

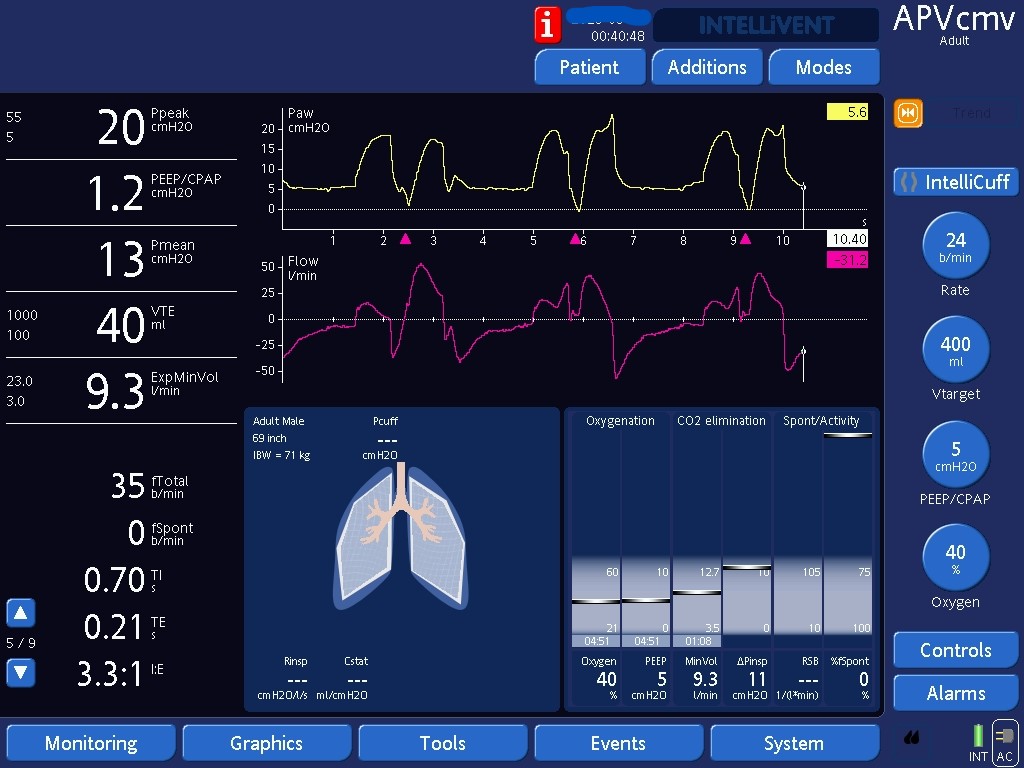
Flow dyssynchrony increases work of breathing and should be corrected when present. Several strategies exist, and the most appropriate one depends on the clinical scenario. One approach is to increase inspiratory flows. On this ventilator, we cannot set flows directly but can increase them by shortening the inspiratory time (iTime). In this example, we decreased the iTime from 1s to 0.7s, which increased flows. Note how the mid-inspiratory deflection in airway pressure is less evident. If the high respiratory drive is due to low tidal volumes, one could attempt increasing tidal volumes. With a constant iTime, higher tidal volumes increase flows. Alternatively, placing the patient on a pressure-limited mode where the patient has more control over inspiratory flows could be attempted, but typically tidal volumes will also increase. If lung protective ventilation demands low tidal volumes, the best next step would be increasing sedation to take away the demand for high flows/volumes.