Effects of Respiratory Effort on Waveforms
How inspiratory effort affects airway pressure and flow waveforms in pressure-limited modes.
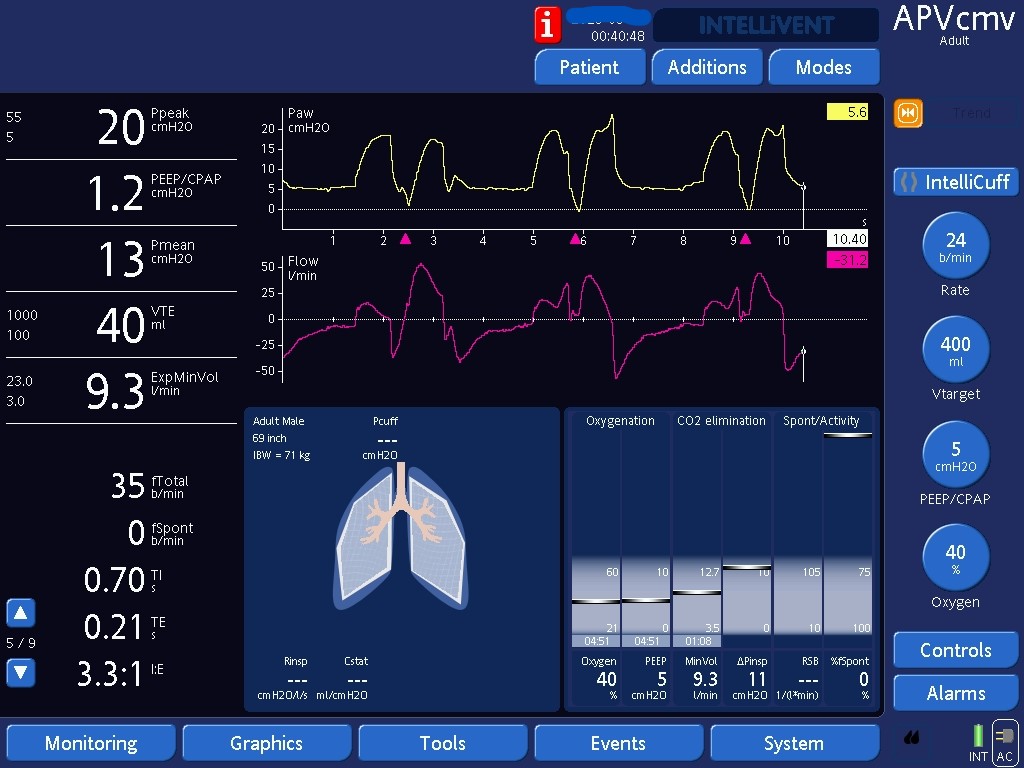
This picture demonstrates the characteristic effects that inspiratory effort (Pimus) has on waveforms in pressure-limited modes (i.e., pressure is the variable controlled by the ventilator whereas flows are the dependent variable). Inspiratory muscles expand the chest, dropping intrathoracic pressures. The drop in intrathoracic pressures is transmitted to the alveoli and airways, driving inspiratory flows and dropping airway pressures. Hence, Pimus will: 1) lower airway pressures from the expected rectangular shape in passive patients, and 2) raise inspiratory flows from the expected upward concavity in passive patients. Compare these waveforms to the waveforms seen in the next picture in another patient on a pressure-limited mode, but who was passive.
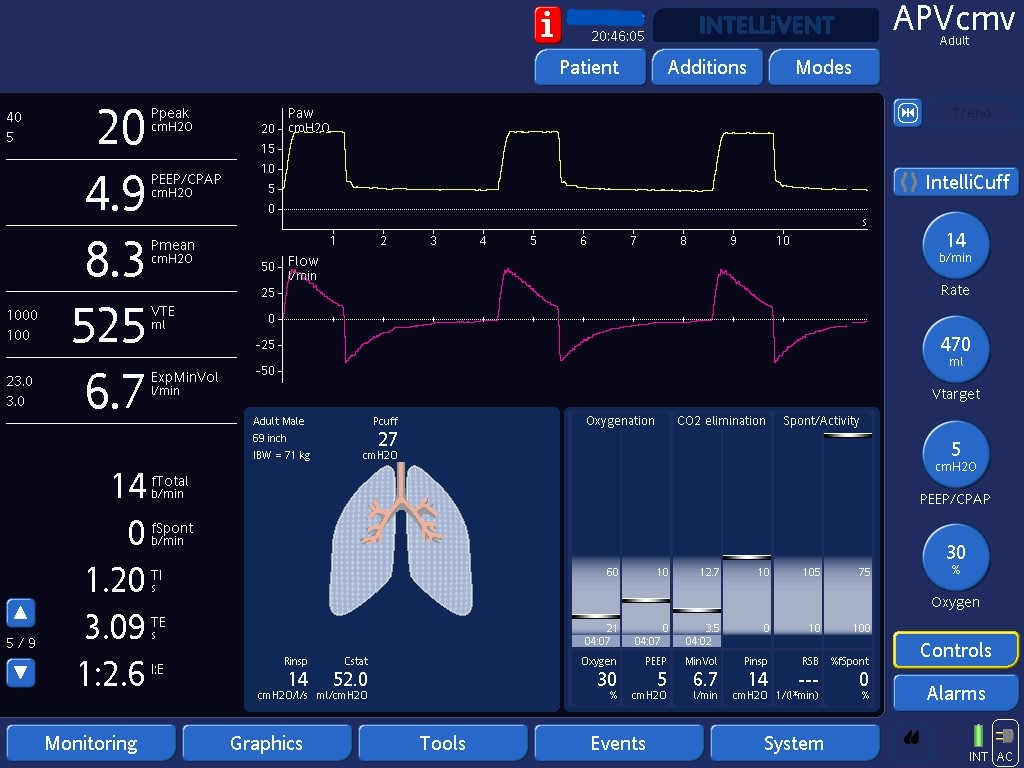
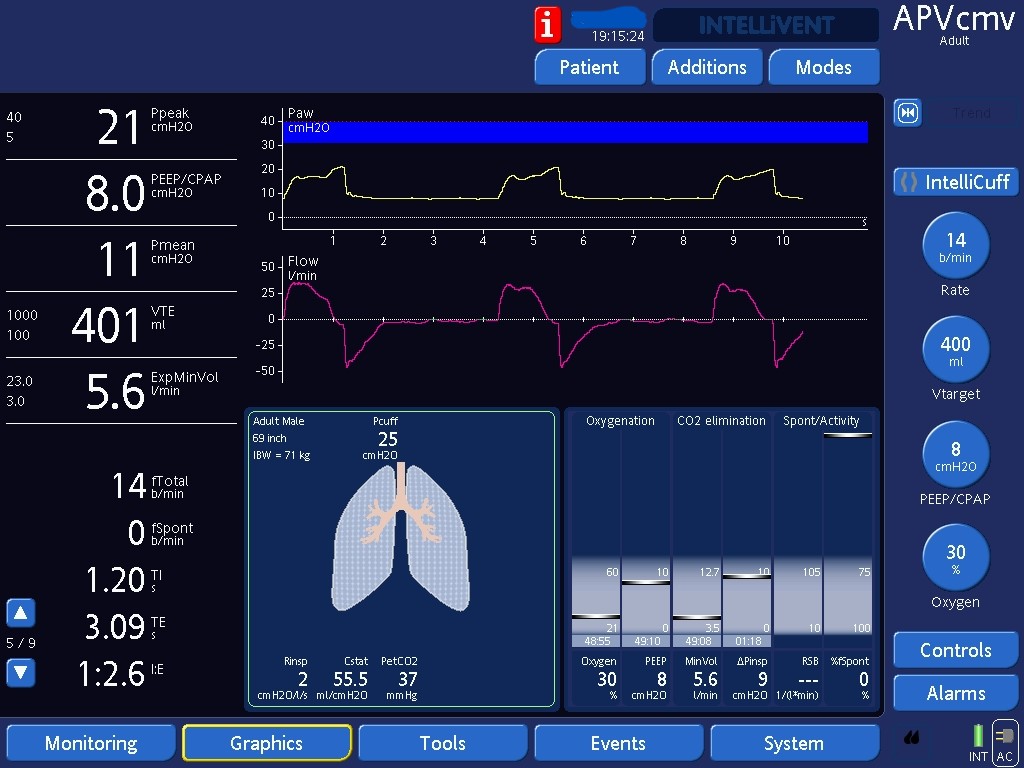
This picture shows the typical shape of passive waveforms in modes where pressure is the controlled variable in inspiration: Airway pressure: has a typical rectangular shape. Airway pressure (Paw) goes from PEEP to peak, stays at peak for duration of inspiration then goes back to PEEP. Inspiratory Flow: Flows are driven by the gradient between airway and alveolar pressures (Paw and Palv). Flows are high at the start of inspiration since Paw just rose to peak and Palv is low, at total PEEP. As inspiration progresses, Paw does not change but, since alveoli inflate, Palv rises. As Palv rises, flows drop. In passive patients, flows drop in an exponential decay pattern, which will give an upward concavity to inspiratory flows. Expiratory flows follow a similar pattern than inspiratory flows. Early expiratory flows are high since Palv is elevated (alveoli are filled with tidal volumes) and Paw has decreased back to PEEP. As the lungs deflate, Palv drops, so expiratory flows progressively decrease. In passive patients, expiratory flows also show an exponential decay pattern with now a downward concavity to the waveform.