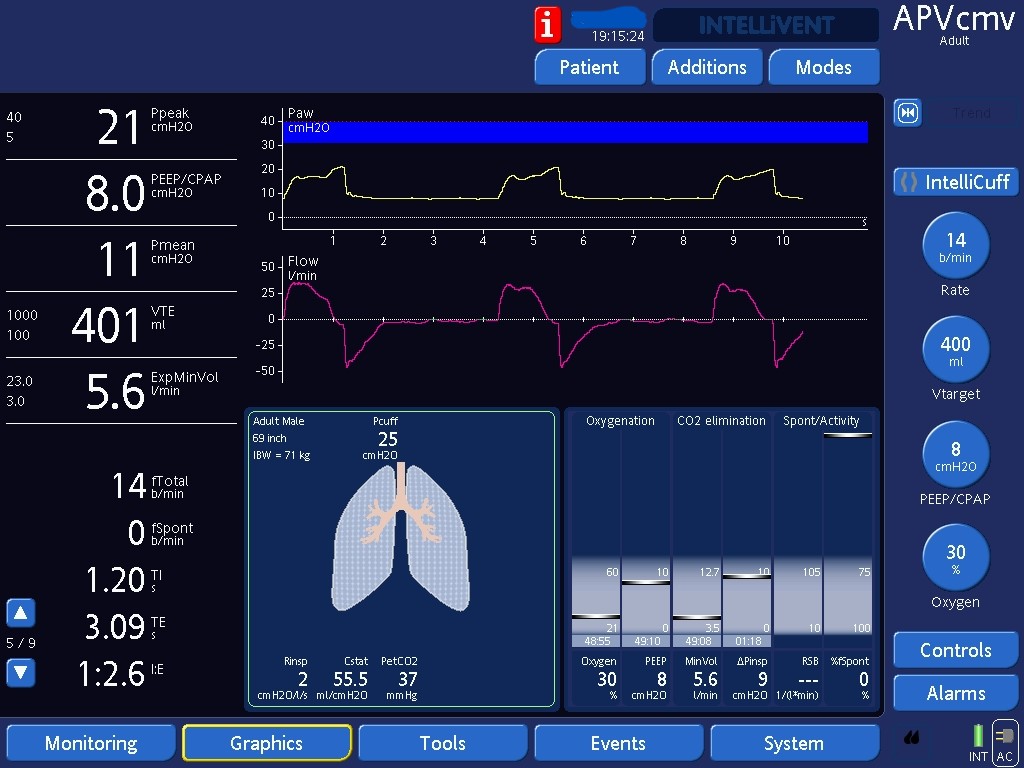
Early Trigger and Troubleshooting Options
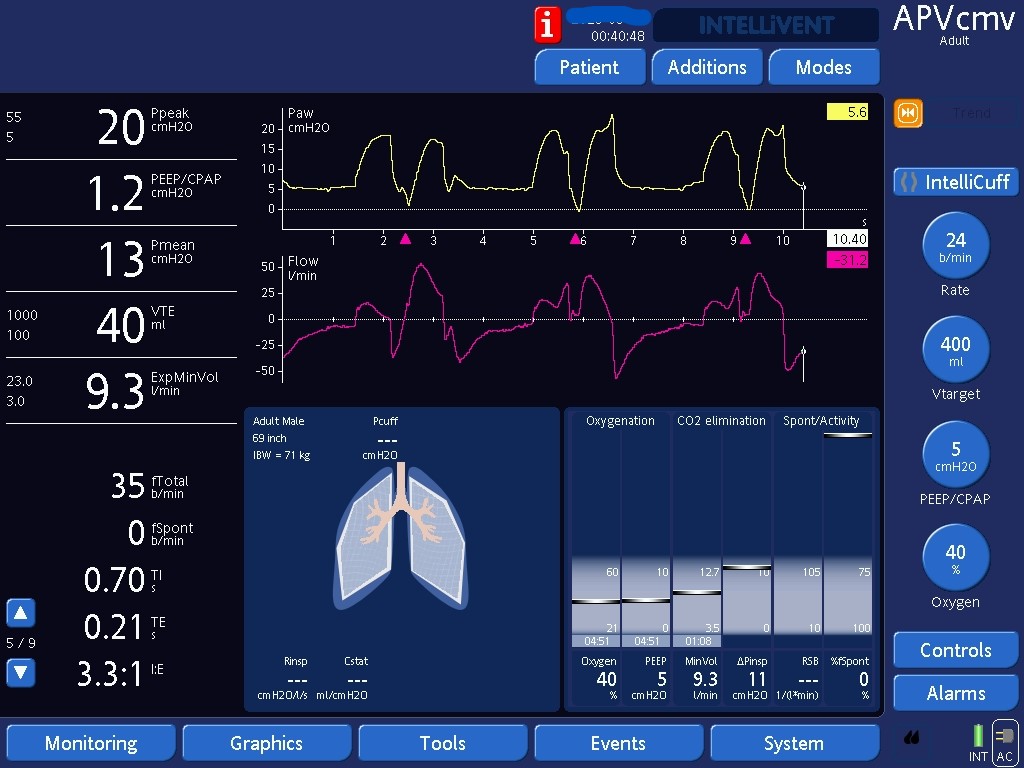
Recognizing early triggering, and two ways to resolve it: dropping the set rate or switching to pressure support.

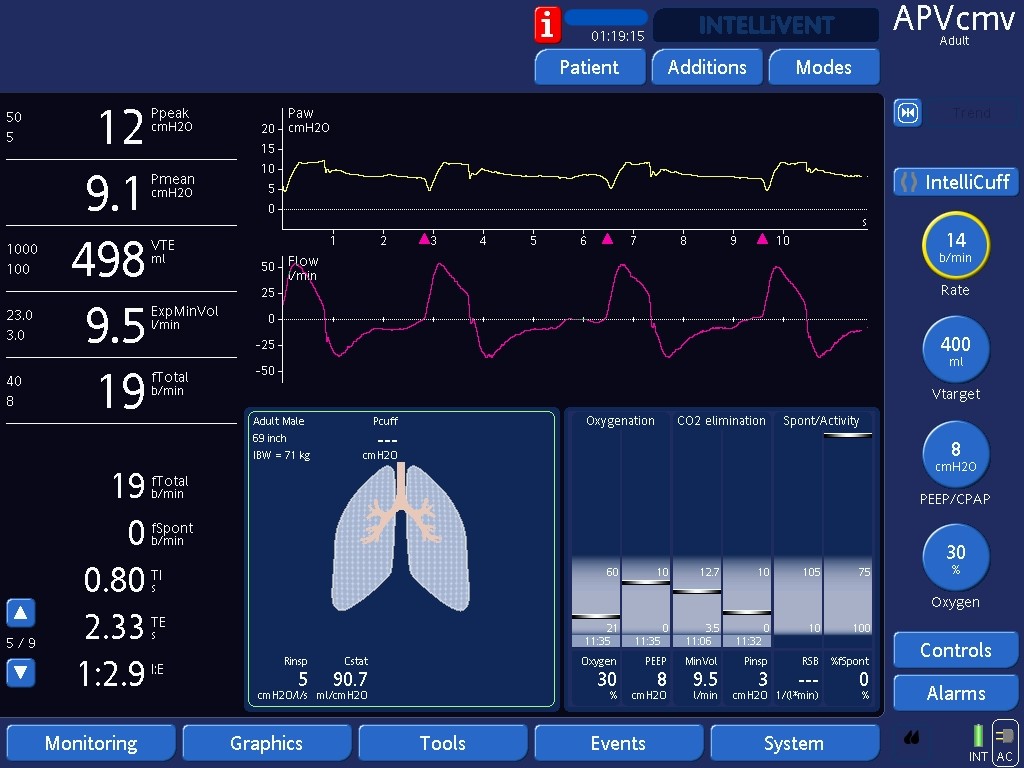
By dropping the set rate, the patient is able to trigger breaths before the ventilator does so, abolishing the phenomenon of early triggering. When clinically acceptable, dropping the set rate is an effective way of treating early triggering; decreasing sedation is often needed to safely drop the set rate. Note how the ventilator only gives 3cmH2O above PEEP (Pinsp in the right lower corner) with each breath in this patient on APV - see next image and further cases below on Work Shifting.
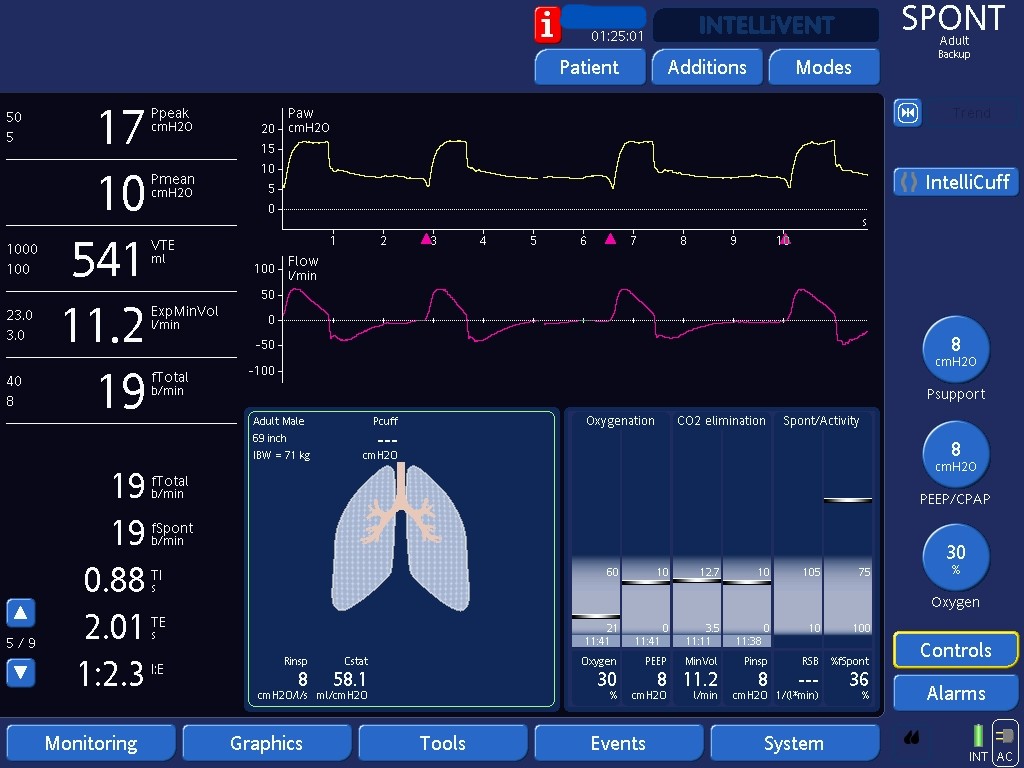
Since early trigger requires that the ventilator triggers a breath before the patient would trigger, pressure support also abolishes early triggering since there are no ventilator-triggered breaths. Note that this patient is better supported on pressure support than on APV since we are now setting the pressure applied above PEEP to 8 cmH20.