Early cycle in VC
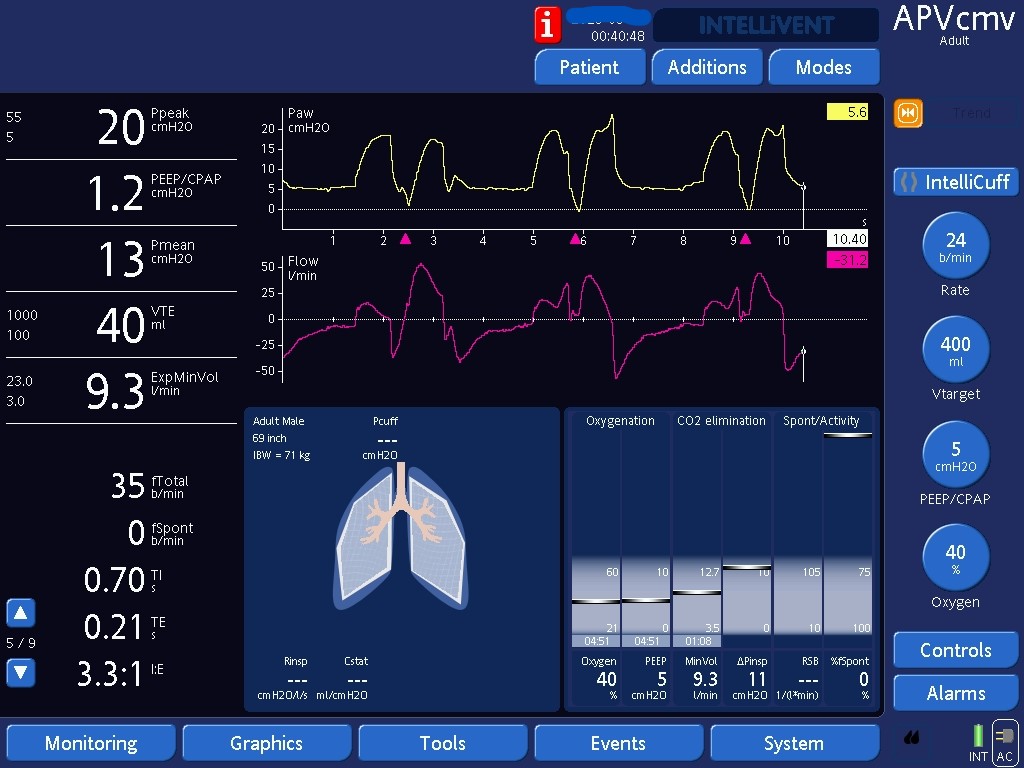
Identifying early cycling in volume control, where inspiratory effort extends past the set inspiratory time into expiration.

Identifying early cycling in volume control, where inspiratory effort extends past the set inspiratory time into expiration.